

Have you noticed worrisome changes in your aging parent?
Maybe they’ve been mostly okay but now you’re seeing problems with memory, such as forgetfulness or asking the same questions repeatedly. Or maybe you’ve noticed trouble with driving, keeping up the house, managing stairs, or paying bills.
Some aging parents simply begin to seem more withdrawn. Others start leveling accusations at others, claiming someone took or moved something, or acting paranoid.
For many adult children, these changes lead to mounting questions. What’s wrong? What’s happening? Is it safe for Mom to keep driving? Should Dad live alone much longer?
I think of this as the “uh-oh” stage. It’s a transition no one looks forward to, and most haven’t prepared for: the time when you might have to start helping your aging parent.
And for many, it comes with an added challenge: Most aging parents don’t welcome much help from their adult children. They may see it as interference, or an invasion of privacy.
Some parents might even refuse to accept that they’re having difficulties, despite issues that feel glaringly obvious—and concerning—to you.
By the time you’re noticing changes and have safety concerns, it’s quite possible that you’re right: that your parent does need help of some kind. So how should you best get involved, especially if your attempts to do so have gone poorly in the past?
Well, it’s certainly not easy. These situations are complicated from a medical and eldercare perspective, plus they tend to bring up difficult emotions for older parents and adult children alike.
But I do believe that it’s crucial for families to get involved. It’s not likely to be easy. But it can be easier, if you’re able to learn the better ways to do so—and also what to stop doing.



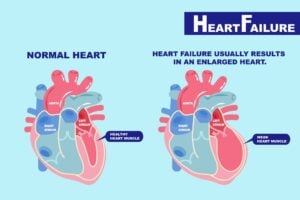 Have you been told that you — or someone important to you — has heart failure?
Have you been told that you — or someone important to you — has heart failure?


 Have you ever wondered how diabetes (or prediabetes) affects older adults?
Have you ever wondered how diabetes (or prediabetes) affects older adults?
